
Summary
This article reviews premenopause, perimenopause, menopause, and postmenopause, discusses how hormonal changes impact symptoms, and explores clinical strategies, including bioidentical hormone therapy.
Introduction
“one-third of U.S. OB/GYN residency programs offer a standardized menopause curriculum”
Menopause is a universal biological transition, but its presentation can be unpredictable. Despite its prevalence, menopause education remains underrepresented in medical training and lacks consistency in clinical care. A national survey published in Menopause found that roughly one-third of U.S. OB/GYN residency programs offer a standardized menopause curriculum, and even fewer provide hands-on menopause-specific training [1].
That means many clinicians are expected to guide women through a life stage they were never formally trained to manage, leaving some women underdiagnosed or undertreated during one of the most transformative phases of their lives. This article explores each stage of menopause, standard and emerging therapy considerations, and bioidentical hormones (BHRT).
Understanding the Stages of Menopause
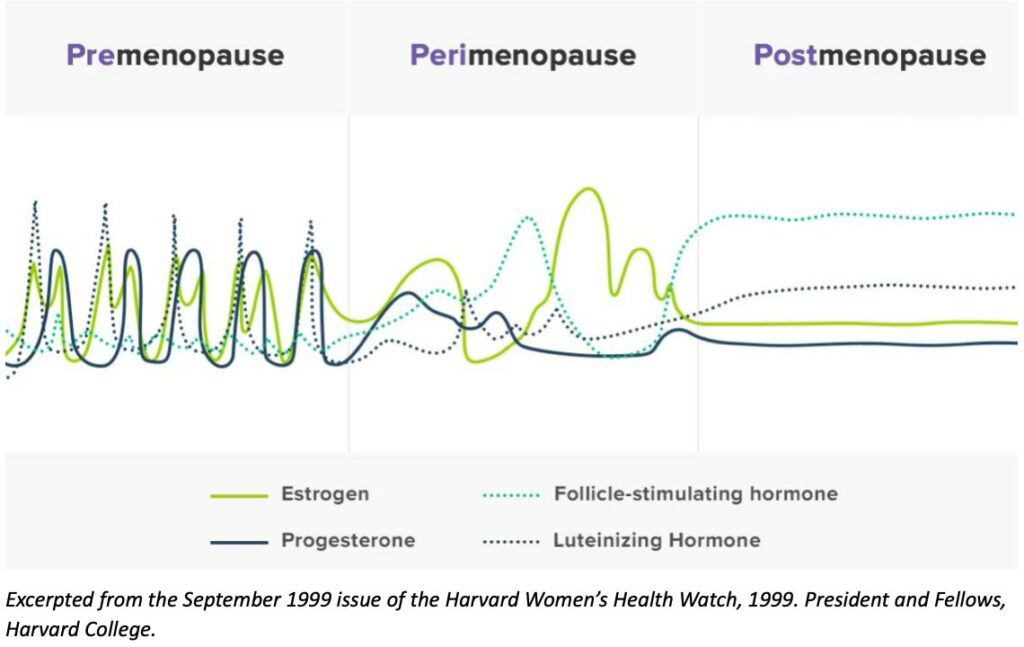
Clinically, menopause is defined as a single event: the point when a woman has gone twelve consecutive months without a menstrual period, marking the end of reproductive function. While this milestone is important diagnostically, it is not the start or end of the hormonal transition. These hormonal changes unfold in four connected phases: premenopause, perimenopause, menopause, and postmenopause, each with distinct hormonal patterns, symptoms, and treatment needs.
Premenopause: The Reproductive Years
Premenopause includes the reproductive years when ovulation is regular, and hormone cycles are relatively stable. However, conditions such as PMS and PCOS can still emerge during this time, often due to progesterone insufficiency or estrogen dominance.
“progesterone can help alleviate mood changes, sleep disruption, and, in some cases, cyclic migraines”
Research shows that micronized bioidentical progesterone can help alleviate mood changes, sleep disruption, and, in some cases, cyclic migraines by acting on GABA-A receptors in the brain [2]. For patients with PCOS, cyclic progesterone may help regulate endometrial shedding, improve cycle regularity, and reduce estrogen dominance [3,4].
Importantly, micronized bioidentical progesterone is chemically identical to the body’s own progesterone and should not be confused with synthetic progestins, such as medroxyprogesterone acetate (MPA), which carry higher risk profiles [5]. As hormonal rhythms begin to shift, women quietly enter the next stage, perimenopause.
Perimenopause: The Onset of Hormonal Instability
Perimenopause often begins earlier than patients expect. Progesterone levels begin to decline causing noticeable symptoms to emerge often by the mid-30s and become more common into the late 40s. During this stage, ovulation becomes inconsistent, progesterone steadily decreases, and estrogen levels spike and drop unpredictably [6, 7]. For clinicians, early awareness can lead to more timely diagnosis and management.
“compounded bioidentical estrogens and progesterone allow gradual dose adjustments”
Symptoms in perimenopause can be highly variable and may include hot flashes, disrupted sleep, brain fog, irregular cycles, and mood changes. Because symptoms can shift rapidly, treatment should be flexible and individualized. Low-dose estrogens and micronized progesterone, particularly in compounded bioidentical formats, allow gradual dose adjustments to match evolving needs.
Menopause: The Biological Turning Point
Menopause is confirmed when a woman has gone 12 consecutive months without menstruation, signaling persistently low ovarian estrogen and progesterone. In the U.S., the average age of onset is 51, though genetics, surgical history, or chronic conditions can cause earlier or later onset [8].
After menopause is reached, symptoms often persist, including hot flashes, vaginal dryness, cognitive changes, and poor sleep. This is also a turning point for bone density and cardiovascular health, as estrogen’s protective effects wane [9]. For women with a uterus, systemic estrogen therapy must be paired with progesterone to protect the endometrium [10].
“Many providers choose to use topical estriol and estradiol in a ratio of 80:20 or 50:50″
Vaginal estrogen remains a first-line option for treating genitourinary syndrome of menopause (GSM). These provide targeted relief with minimal systemic absorption [11]. Topical hormone therapies continue to grow in popularity among patients and providers alike. Many providers choose to use topical estriol and estradiol in a ratio of 80:20 or 50:50. They provide effective symptom management while avoiding first-pass hepatic metabolism, which reduces thrombotic risk compared to oral options [12].
Postmenopause: Long-Term Health and Hormone Deficiency
“estrogen deficiency accelerates bone loss and increases cardiovascular vulnerability”
Postmenopause begins immediately after menopause is confirmed and continues for the rest of a woman’s life. For some, the more disruptive symptoms fade, while others continue to experience vaginal dryness, urinary discomfort, low libido, or lingering hot flashes. Estrogen deficiency at this stage also accelerates bone loss and increases cardiovascular vulnerability.
When started early in healthy women under 60, hormone therapy can help preserve bone density and reduce cardiovascular risk [13]. DHEA supplementation may also support mood, libido, and energy [14]. There is also substantial evidence supporting the use of testosterone in women though access to it remains an unmet need [15].
Holistic evaluation is critical, including comprehensive labs, symptom tracking, and patient-reported outcomes. Even when hormone levels appear “normal,” functional imbalances may still cause symptoms.
Conclusion
Menopause is a single event, yet it occurs within a larger continuum of hormonal changes that affect women before and long after their final menstrual period. Each stage presents unique symptoms and health considerations that require individualized management. Clinicians play a vital role in helping patients recognize early signs, understand treatment options, and access therapies that support both symptom relief and long-term wellness. Evidence-based approaches can offer safe and flexible solutions. By combining clinical expertise with patient-centered care, providers can guide women confidently through this transformative life stage. At every stage of menopause, Carie Boyd Pharmaceuticals provides trusted treatment options and support to help you deliver the best care for your patients. Check out or hormone creams, oral hormones, and adjunctive hormone therapies.
Coming Soon...
Stay tuned for our next article that discusses the Women’s Health Initiative Study, the July 2025 FDA Expert Panel on Menopause and Hormone Replacement Therapy, and bioidentical hormones!
- Faubion, S. S., et al. (2023). Needs assessment of menopause education in United States obstetrics and gynecology residency training programs. Menopause, 30(9), 1011–1018. https://doi.org/
- Prior JC. Progesterone for treatment of symptomatic menopausal women. Climacteric. 2018 Aug;21(4):358-365. doi: 10.1080/13697137.2018.1472567. Epub 2018 Jul 2. PMID: 29962247.
- Shirin S, Murray F, Goshtasebi A, Kalidasan D, Prior JC. Cyclic Progesterone Therapy in Androgenic Polycystic Ovary Syndrome (PCOS)-A 6-Month Pilot Study of a Single Woman’s Experience Changes. Medicina (Kaunas). 2021 Sep 26;57(10):1024. doi: 10.3390/medicina57101024. PMID: 34684061; PMCID: PMC8538639.
- Dr. Reddy’s Laboratories, Inc. (2024, March). Progesterone capsules, 100 mg and 200 mg [Prescribing information]. https://dailymed.nlm.nih.gov/
- Holtorf K. The bioidentical hormone debate: are bioidentical hormones (estradiol, estriol, and progesterone) safer or more efficacious than commonly used synthetic versions in hormone replacement therapy? Postgrad Med. 2009 Jan;121(1):73-85. doi: 10.3810/pgm.2009.01.1949. PMID: 19179815.
- Lyndaker C, Hulton L. The influence of age on symptoms of perimenopause. J Obstet Gynecol Neonatal Nurs. 2004 May-Jun;33(3):340-7. doi: 10.1177/0884217504264872. PMID: 15180197.
- Prior JC, Hitchcock CL. The endocrinology of perimenopause: need for a paradigm shift. Front Biosci (Schol Ed). 2011 Jan 1;3(2):474-86. doi: 10.2741/s166. PMID: 21196391.
- USPSTF. Postmenopausal hormone replacement therapy for the primary prevention of chronic condition. Recommendations and rationale. U.S. Preventive Services Task Force. Am Fam Physician. 2003 Jan 15;67(2):358-64. PMID: 12562158.
- Salpeter SR, Walsh JM, Greyber E, Ormiston TM, Salpeter EE. Mortality associated with hormone replacement therapy in younger and older women: a meta-analysis. J Gen Intern Med. 2004;19(7):791-804. doi:10.1111/j.1525-1497.2004.30281.x
- Harper-Harrison G, Carlson K, Shanahan MM. Hormone Replacement Therapy. [Updated 2024 Oct 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/
- Academic Committee of the Korean Society of Menopause, Lee SR, Cho MK, et al. The 2020 Menopausal Hormone Therapy Guidelines. J Menopausal Med. 2020;26(2):69-98. doi:10.6118/jmm.20000
- Bagot CN, Marsh MS, Whitehead M, Sherwood R, Roberts L, Patel RK, Arya R. The effect of estrone on thrombin generation may explain the different thrombotic risk between oral and transdermal hormone replacement therapy. J Thromb Haemost. 2010 Aug;8(8):1736-44. doi: 10.1111/j.1538-7836.2010.03953.x. Epub 2010 Jun 14. PMID: 20553380.
- Hodis HN, Mack WJ. Menopausal Hormone Replacement Therapy and Reduction of All-Cause Mortality and Cardiovascular Disease: It Is About Time and Timing. Cancer J. 2022 May-Jun 01;28(3):208-223. doi: 10.1097/PPO.0000000000000591. PMID: 35594469; PMCID: PMC9178928.
- Rutkowski K, Sowa P, Rutkowska-Talipska J, Kuryliszyn-Moskal A, Rutkowski R. Dehydroepiandrosterone (DHEA): hypes and hopes. Drugs. 2014 Jul;74(11):1195-207. doi: 10.1007/s40265-014-0259-8. PMID: 25022952.
- Parish SJ, Simon JA, Davis SR, Giraldi A, Goldstein I, Goldstein SW, Kim NN, Kingsberg SA, Morgentaler A, Nappi RE, Park K, Stuenkel CA, Traish AM, Vignozzi L. International Society for the Study of Women’s Sexual Health Clinical Practice Guideline for the Use of Systemic Testosterone for Hypoactive Sexual Desire Disorder in Women. Climacteric. 2021 Dec;24(6):533-550. doi: 10.1080/13697137.2021.1891773. Epub 2021 Apr 1. PMID: 33792440.